


BICARICU-2: Sodium Bicarbonate reduces need for renal replacement but does not change mortality.
- Martin Cearras, MD
- Dec 16, 2025
- 2 min read

Find the original article here!
Summary:
This trial is a follow up to the BICARICU trial which suggested that targeted use of sodium bicarbonate in critically ill patients with metabolic acidemia may offer survival and less renal replacement therapy. BICARICU-2 is a French open label RCT, that enrolled 640 ICU patients from 43 ICUs. Included patients presented with severe metabolic acidosis and severe AKI. Both per protocol and ITT analyses were performed. Primary outcome of mortality was not different, renal replacement need was again lower in the intervention group with a NNT of 7. All other secondary outcomes and adverse effects were similar in both groups.
PICOTT:
Population: ICU patients with severe metabolic acidosis and severe AKI.
Intervention: IV 4.2% sodium bicarbonate to target a pH > 7.3 for 28 days or until ICU discharge
Comparison: Nothing (No placebo)
Outcomes: Primary: 90 day mortality
Type of Question: Therapy
Type of Study: RCT
Interpretation of the Study:
Unsurprisingly, there is no difference in mortality with the administration on sodium bicarbonate. The reduction in renal replacement therapy (RRT) need makes sense, as acidemia is an indication for RRT. Once RRT is started, patients are less likely to be RRT free at 28 days.
Sodium Bicarbonate is a safe, cheap intervention that has consistently helped avoid RRT in critically ill patients.
All the other secondary outcomes are hypothesis generating and should be treated as such.
Surprisingly, the overall mortality in both groups (62%) is higher than expected for septic shock patients in other studies (~30% average). 30% of patients were in surgical ICUs, which have an even lower mortality.
-The ARR for RRT is 15% (50% CER - 35% EER) with a NNT of 7, consistent with the findings of BICARICU-1.
Overall Risk of bias:
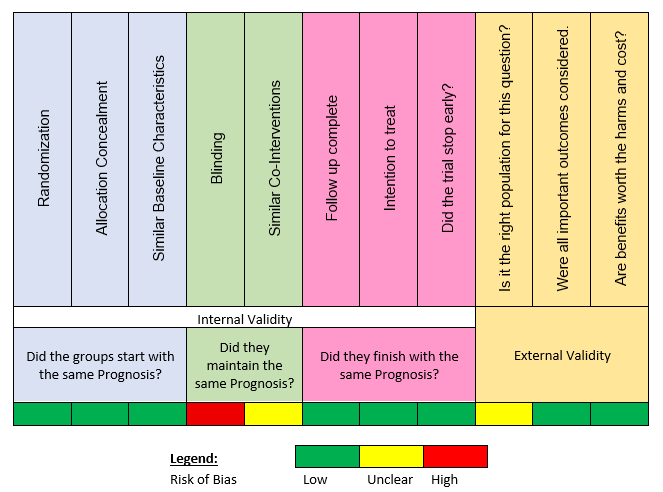
Pros: both ITT and per protocol analyses were done. Results were similar, adding strength to them.
Cons: The trial was open-label and there was no placebo. There were 47 patients in the control group that crossed over to the experimental group. This is problematic and likely worsened the outcomes seen in the experimental group, as crossovers tend to be sicker than the other
patients (however, not clearly seen on the supplements, as groups seem similar).
Context:
Data is similar to what we previously thought about use of sodium bicarbonate in the ICU and the importance of avoiding RRT when possible (BICARICU-1, STARRT AKI).
Teaching points:
Outcome measures
Relative risk and Risk difference (ARR)
NNT (number needed to treat)
Intention-to-treat analysis vs. per-protocol/as-treated analysis
Blinding
Verdict:
Somewhat settled - Might change with more data


Comments